
Quantifying inspiratory effort can be useful in many aspects of assisting a person that is undergoing mechanical ventilation. For example, it represents the first step in understanding whether the level of pressure support set in the ventilator is adequate for the clinical objective or the importance of this data in the early detection of Patient Self Inflicted Lung Injury (P-SILI).
A normal or acceptable level of respiratory effort during mechanical ventilation is generally described as:
- Muscle pressure (Pmus) has to be between 5 e 10 cmH2O [1];
- Pressure time product (PTP) has to be between cmH2O·s·min-1 [1-3];
- Work of breathing (WOB) has to be between 2,4 e 7,5 J·min-1 o 0,2 e 0,9 J·L-1 [4].
This data is used extensively in research, but it’s difficult, almost impossible, to monitor in a clinical setting [5].
So now the question is: without advanced monitoring, can inspiratory effort be reliably measured at the patient’s bed?
The parameters that help us with more or less precision in this monitoring are:
- P 0,1
- PMI
- Flow Index
- ∆Pes
P 0,1
This represents the negative change in airway pressure generated by an end-expiratory occlusion during the first 100 ms of an inspiratory effort (image 1). It is used as an indicator of the central respiratory drive [6], which is the level of activation of the breath center. During this process, the greater the respiratory drive, the greater the force with which the respiratory muscles contract, which will result in the depression generated against the occluded airway [7].
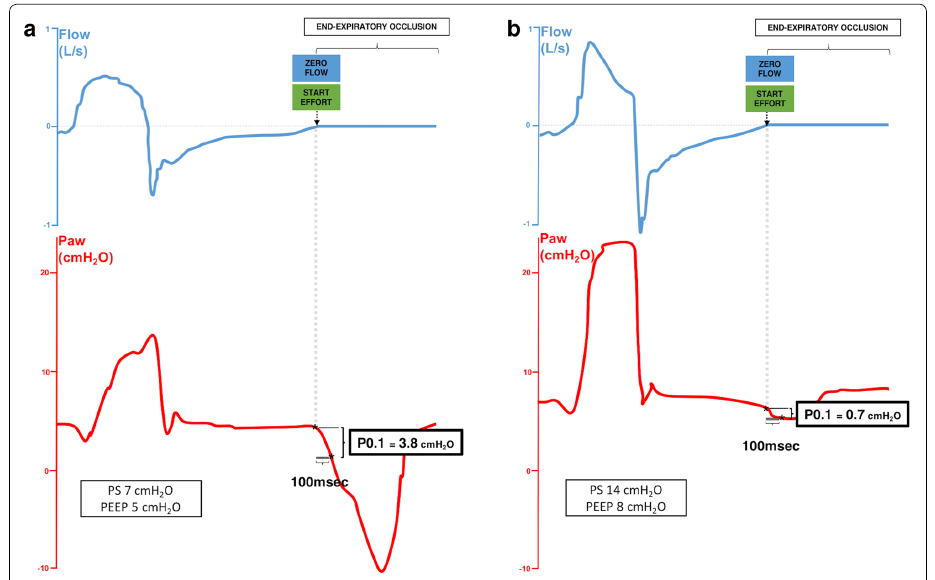
During assisted mechanical ventilation P 0,1 value lower than 1,6 cmH2O indicates low respiratory drive and as a result, may suggest an inadequate respiratory effort [9]. Lower values may occur when there is excessive ventilator assistance, muscle weakness, or high sedation level. P 0,1 > 3,5 cmH2O values (indicators of an elevated Drive) correlate with excessive inspiratory effort with a sensitivity of 80% to 92% and a specificity of 77% to 89% [5]. P 0,1 value is underestimated in patients that present an intrinsic peep. It is important to make an average of 3-5 values as the P0,1 varies with it each patient’s breath.
Some ventilators (examples: Servo-I, Getinge Solna) estimate the value based on the drop in airway pressures during the beginning of the trigger phase (the value is automatically provided with each respiratory act). The other model shows the measurement that is being performed but only upon operator request.
PMI (Pressure Muscle Index)
The ventilator’s goal during PSV is to maintain a pressure level above PEEP. As a result, the more force the muscles exert during inspiration, the greater the flow delivered by the ventilator. The increase in flow results in an increase in volume and a consequent increase in end-inspiratory alveolar pressure (Pplat). [10]
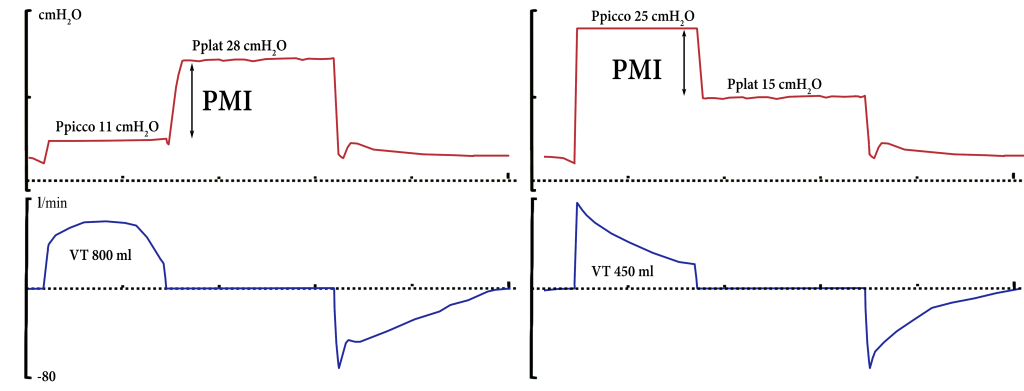
The difference between plateau (Pplat or pause of end-inspiration) and expected peak pressure (PEEP + PS) is called PMI. This value can provide an estimate (approximate by default) of the muscle force exerted by the patient (Pmus).
PMI = Pplat – (PS + PEEP)
A PMI > 6 cmH2O may indicate intense inspiratory muscle work (in respiratory systems with normal resistance) [11]. A PMI < 2 cmH2O or even a negative value may indicate a complete transfer of work of breathing on the ventilator indicating over-assistance. Image 2 shows an example of the PMI measurement during PSV.
Recent studies suggest that excessive inspiratory effort during PSV cannot be quantified precisely by the PMI. This approach, on the other hand, proves to be extremely accurate for the screening of subjects at risk of absence or minimal activation of the respiratory muscles and, therefore, for preventing ventilator-induced diaphragmatic dysfunction. [12]
It’s very important always to remember that the PMI evaluates only the final inspiration effort and not the total effort during inspiration, because it does not take into account the inspiratory resistive load. It is also important to know that PMI can only be linked to respiratory activity that is developed after the flow onset: what happens before the activation of the trigger, does not produce an increase in lung gas volume, and does not affect the plateau pressure. Therefore, it cannot be excluded that the patient made a significant effort to exceed the threshold load of the self-generated PEEP.
Flow index
A continuous evaluation of the inspiratory workload of the muscle is possible by observing the flow index or the morphology of the inspiratory flow wave [13].
The flow index numerically describes the concavity of the wave:
- Flow index = 1 when inspiratory flow decreases linearly.
- Flow index < 1 describes away form with an upward-facing concavity.
- Flow index > 1 if the curve has a downward concavity.
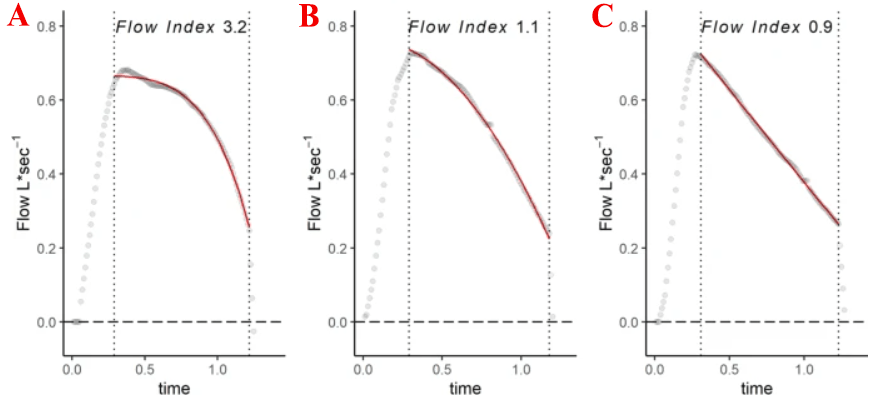
In this model, the inspiratory flow is a function of the peak flow time (a), the rate of flow reduction (b), and the c parameter, which describes the downward pointing concavity of the declining phase of the inspiratory flow wave. The c parameter is the Flow Index. Image from Albani F, et al 2021. [13]
If the wave after the initial peak decreases linearly (image 3 C) or shows an exponential decline (upward concavity) it can be said that the force exerted by the respiratory muscle is minimal or absent; if the wave has a downward concavity or sinusoidal aspect, it can be assumed that the inspiratory work is carried out in part or totally by the patient.
Evidence today shows that thanks to the flow index it is possible to evaluate whether the work of breathing is more dependent on the ventilator or the respiratory muscles. It is not, however, defined a cut-off that establishes whether the inspiratory effort is normal or excessive. [13]
To give a simple example of the use of the flow index in daily practice, we propose to opposite situations
- If, after reconnecting the patient to the ventilator, (example: Spontaneous breathing trial) a respiratory pattern is characterized by intense work of breathing (sinusoidal wave), it is advised to warn the doctor and evaluate the increase of inspiratory assistance to let the muscles rest.
- If the patient has a decreasing inspiratory flow, it is important to evaluate the possibility of reducing the pressure support and allowing the patient to work, using the diaphragm, to prevent ventilator-induced diaphragmatic dysfunction (VIDD).
∆Pes
The gold standard in assessing respiratory effort is esophageal pressure (Pes). Using an esophageal catheter, it is possible to accurately estimate the change in pleural pressure during respiration. The inspiratory oscillation of esophageal pressure (∆Pes) is very easy to measure (monitored continuously) in the end it’s done at the bedside and can be viewed directly on the screen of some ventilators (ex: Hamilton G5 and C6).
The PES absolute value is approximately 2 ± 1 cmH2O which is inferior to the absolute value of Pmus. Therefore, monitoring allows the detection of inappropriate inspiratory efforts with extreme accuracy [5], taking into account all the forces that the muscles must overcome during inspiration: threshold load, elastic load, and resistive load.
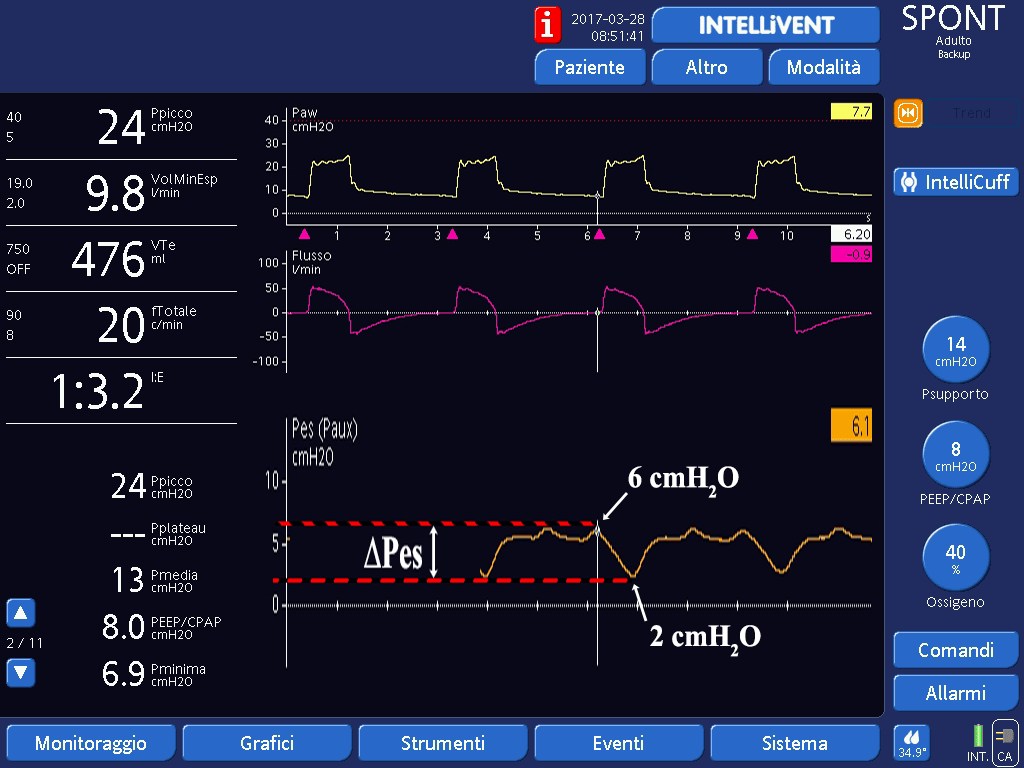
An absolute ∆Pes value above < 2 o 3 cmH2O is generally considered a sign of overexertion of muscle weakness or elevated doses of sedation. An absolute ∆Pes value greater than 10-12 cmH2O is considered a marker of under-assistance and/ or excessive inspiratory effort [14].
Image 4 shows the esophageal pressure wave (orange) of a patient with normal inspiratory muscle activation (lower limit).
Thank you
Enrico Bulleri
English version edited by Giulia Azzini
Bibliography
- Mauri T., Yoshida T., Bellani G., Goligher E., Carteaux G., Rittayamai N., Mojoli F., Chiumello D., Piquilloud L., Grasso S., et al. Esophageal and Transpulmonary Pressure in the Clinical Setting: Meaning, Usefulness and Perspectives. Intensive Care Med. 2016;42:1360–1373.
- Carteaux G., Mancebo J., Mercat A., Dellamonica J., Richard J.-C.M., Aguirre-Bermeo H., Kouatchet A., Beduneau G., Thille A.W., Brochard L. Bedside Adjustment of Proportional Assist Ventilation to Target a Predefined Range of Respiratory Effort. Crit. Care Med. 2013;41:2125–2132.
- Beck J., Gottfried S.B., Navalesi P., Skrobik Y., Comtois N., Rossini M., Sinderby C. Electrical Activity of the Diaphragm during Pressure Support Ventilation in Acute Respiratory Failure. Am. J. Respir. Crit. Care Med. 2001;164:419–424.
- Akoumianaki E., Maggiore S.M., Valenza F., Bellani G., Jubran A., Loring S.H., Pelosi P., Talmor D., Grasso S., Chiumello D., et al. The Application of Esophageal Pressure Measurement in Patients with Respiratory Failure. Am. J. Respir. Crit. Care Med. 2014;189:520–531.
- Carteaux G, Parfait M, Combet M, Haudebourg AF, Tuffet S, Dessap AM. Patient-Self Inflicted Lung Injury: A Practical Review. J Clin Med. 2021; 10 (12): 2738.
- Vaporidi K., Akoumianaki E., Telias I., Goligher E.C., Brochard L., Georgopoulos D. Respiratory Drive in Critically Ill Patients. Pathophysiology and Clinical Implications. Am. J. Respir. Crit. Care Med. 2020;201:20–32.
- http://www.ventilab.org/2013/05/20/p0-1-pressione-di-occlusione-delle-vie-aeree-cosa-e-come-utilizzarla.
- Telias I, Damiani F, Brochard L. The airway occlusion pressure (P0.1) to monitor respiratory drive during mechanical ventilation: increasing awareness of a not-so-new problem. Intensive Care Med. 2018;44:1532–5.
- Bertoni M, Spadaro S, Goligher E.C. Monitoring Patient Respiratory Effort During Mechanical Ventilation: Lung and Diaphragm-Protective Ventilation. Crit Care 2020. 24:106.
- Bulleri E, Fusi C. Guida al monitoraggio della ventilazione meccanica. Triggerlab edizioni. Como 2020.
- Foti G et al. End-inspiratory airway occlusion: a method to assess the pressure developed by inspiratory muscles in patients with acute lung injury undergoing pressure support. Am J Respir Crit Care Med 1997;156:1210–1216.
- Natalini G, Buizza B, Granato A, Aniballi E, Pisani L, Ciabatti G, et al. Non-invasive assessment of respiratory muscle activity during pressure support ventilation: accuracy of end-inspiration occlusion and least square fitting methods. J Clin Monit Comput. 2020, 2: 1–9.
- Albani F, Pisani L, Ciabatti G, Fusina F, Buizza B, Granato A, et al. Flow Index: a novel, non-invasive, continuous, quantitative method to evaluate patient inspiratory effort during pressure support ventilation. Crit Care. 2021;25(1):196.
- Goligher E.C., Dres M., Patel B.K., Sahetya S.K., Beitler J.R., Telias I., Yoshida T., Vaporidi K., Grieco D.L., Schepens T., et al. Lung- and Diaphragm-Protective Ventilation. Am. J. Respir. Crit. Care Med. 2020;202:950–961.
