
English version edited by Giulia Azzini, Rn, Intensive Care Unit, Department of Anaesthesiology, Emergency and Intensive Care Medicine (DAEICM), Ente Ospedaliero Cantonale (EOC), Bellinzona, Switzerland.
In order to understand this asynchrony, it is important to know the meaning of ” Entraiment”. In physics, this term defines the phase and the timeline of a periodic external output. In a neuroscientific field, “entrainment” is when the cerebral waves show a superimposable oscillation on a periodic external stimulus. For example, exposure to music can cause a “respiratory entrainment” in the respiratory area of expertise attributed to a permanent and repetitive reaction between neural respiratory cycles distributed by the ventilator.
The results of the studies that have been conducted were performed on sedated animals and on healthy people, while awake and while asleep and during induced anesthesia (1).
Respiratory entrainment was observed for the first time in 2013, in patients in critical care undergoing mechanical ventilation; this type of respiratory pattern has been classified as “reverse triggering”. It consists of diaphragmatic contractions seemingly triggered by the insufflation engaged by the mechanical ventilation with different ratio (1:1; 1:2; 1:3) and phenotypes (premature, medium, tardive) (2,3).
The pathogenesis is still completely unknown and it is thought it may be activated/triggered by the vagal mediation as well as sub-cortical (3) and cortical effects.
Reverse triggering has been frequently recorded in sedated patients affected with ARDS, and lately, it has been observed in patients that suffer brain deaths. (4)
Even though it has not been proven explicitly, the consequences of reverse triggering may provoke the following:
- plyometric diaphragmatic contraction is related to the emission of cytokines and fiber muscular damage that could determine a ventilator-induced diaphragmatic dysfunction (VIDD); (5,6)
- work of breathing and oxygen consumption (7);
- difficult survey of plateau pressure; lung injury by overdistension (volutrauma); (8)
- delayed brain death diagnosis. (4)
Reverse triggering is often confused with other types of asynchronies such as Double-triggering as well as Premature cycling. Unfortunately, it’s difficult even for experts to identify the difference by utilizing exclusively ventilator waveforms. For this reason, the observation of the waves obtained utilizing an esophageal catheter and the ” EAdi catheter” are by far the best way to identify it.
How to identify a Reverse triggering
“Figure 1” shows the waves of a patient undergoing a controlled ventilation setting “Pcv-vg”. As we can see, there are no trigger deflections on the pressure waves, which suggests no participation whatsoever from the patient during the phase of activation of the inspiratory muscles.

The patient’s neural drive is passively stimulated by the ventilator’s insufflation, but the reaction of this stimulation is subject to change, due to temporal activation and muscle intensity.
The image shows the absence of the trigger deflection on the wave pressure. During the mechanical breath it’s evident that a patient tardive response corresponds to the near end of the inspiratory cycle and the tightening respiratory musculature produces a double-triggering that has to be identified as a false double-triggering, specifically that a reverse-triggering has occurred. In fact, it will not activate the first nor the second artificial breath, a characteristic of double-triggering. Reverse triggering is distinguished by a first insufflation it is not activated by the patient, but it is mandated and the patient will only trigger the second mechanical breath. This is the reason of the false double-triggering deflection.
From a clinical point of view, it’s very important to recognize the difference between these asynchronies because the treatment is different for each one (Images 2 and 2.1).
Alterations such as the premature cycling and double-triggering are caused by:
- inadequate inspiratory time;
- excessive patient need/request and/or insufficient volume/pressure support. (The solutions have been previously discussed in the paragraphs above).
When these asynchronies are generated by a reverse triggering, the approach to the solution changes completely; even though the mechanism of activation has not yet been discovered. The 3rd image shows a reverse triggering that lingers within the patient’s breathing inspiratory pattern.
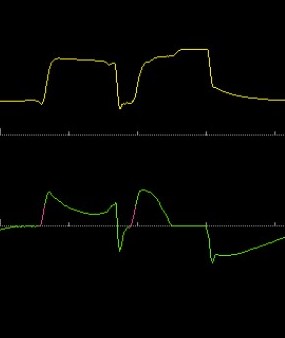
Image 2: example of a double triggering, the trigger deflection is well shown. Image 2.1: example of a false double triggering; there is no trigger deflection, defined as a reverse triggering asynchrony.
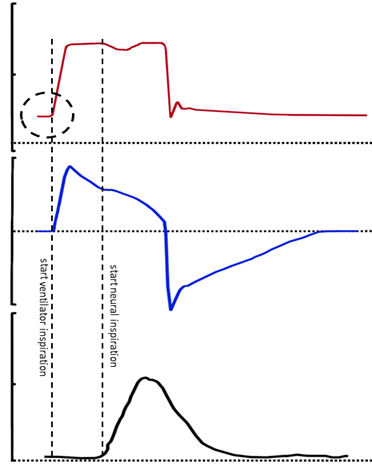
The ventilator launches an insufflation with the timing and settings established, and the patient will activate his/her inspiratory respiratory muscles only a tenth of a second later. The activation is noticeable with a slight deflection on the pressure-time wave, whereas a slight convex will show on the flow-time wave. The third “EAdi” track, is settling clearly showing the discrepancy between the ventilator insufflation and the eventual neural diaphragmatic reaction. In this specific case, the discrepancy doesn’t activate other types of asynchronies, such as a premature cycling and double triggering; the neural delay (shown in the EAdi catheter) remains confined to the inspiratory time.
To this day, the mechanism of reverse triggering needs more research conducted in order to better understand it, making it impossible to suggest a complete resolution for this asynchrony. After analyzing the data published in literature, it is recommended to use a limited dose of sedation.
Recommendation when confronted with reverse triggering
- Understanding the use of oversedation or undersedation. (Thought to be the probable cause known until today);
- assessment in absence of sedation and possible changes that occurred in the neurological system;
- if possible, use the EAdi catheter or esophageal catheter (as discussed, the only use of the waveforms is not enough or conclusive);
Different strategies have been revealed from a few studies and case reports. However, there is very little evidence on the matter and it is very important to examine every case:
- even though elevated PEEP levels seem to pose risk for a reverse triggering, this setting reduces the deleterious effect on an elevated respiratory drive through a more consistent (supply) pressure such as the overdistension phenomenon of “Pendelluft” other that improve the respiratory gas exchange (8);
- low tidal volumes are associated to reverse triggering (2). It has been shown that increasing the tidal volume reduces/stops this asynchrony;
- raising or reducing the respiratory rate until all the respiratory system is triggered by the patient (9);
- when variations of the ventilator settings are not effective or inapplicable due to the safety measures, it is recommended to apply the correct dose of sedation to the neuromuscular blockers. (10)
Thank you for your attention,
Giulia Azzini
Bibliography
- Simon PM, Zurob AS, Wies WM et al. Entrainment of Respiration in Humans by Periodic Lung Inflations. Effect of State and CO(2). Am. J. Respir. Crit. Care Med; 1999, 160 (3), 950-960
- Akoumianaki E, Lyazidi A, Rey N et al. Mechanical ventilation-induced reverse-triggered breaths: A frequently unrecognized form of neuromechanical coupling. Chest 2013; 143:927-38
- Baedorf Kassis E, Su HK, Graham AR et al. Reverse Trigger Phenotypes in Acute Respiratory Distress Syndrome. Am. J. Respi. Crit. Care Med 2021; 203,67-77
- Delisle S, Charbonney E, Albert M et al. Patient-Ventilator Asynchrony Due to Reverse Triggering Occurring in Brain-Dead Patients: Clinical Implications and Physiological Meaning. Am. J. Respi. Crit. Care Med. 2016; 196, 1166-1168
- Gea J, Zhu E, Gàldiz JB et al. Functional consequences of eccentric contractions of the diaphragm. Arch Bronconeumol 2009; 45:68-74
- Goligher EC, Brochard LJ, Reid WD et al. Diaphragmatic myotrauma: A mediator of prolonged ventilation and poor patient outcomes in acute respiratory failure. Lancet Respi Med 2019; 7:90-8
- Chanques G, Kress Jp, Pohlman A et al. Impact of Ventilator Adjustment and Sedation-Analgesia Practices on Severe Asynchrony in Patients Ventilated in Assist-Control Mode. Crit. Care Med. 2013; 41, 2177-2187
- Yoshida T, Nakamura MAM, Morais CCA et al. Reverse Triggering Causes an Injurious Inflation Pattern during Mechanical Ventilation. Am. J. Respi. Crit. Care Med. 2018; 198, 1096-1099
- Mellado Artigas R, Damiani LF, Piraino T et al. Reverse Triggering Dyssynchrony 24H after Initiation of Mechanical Ventilation. Anestesiology. 2021; 134, 760-769
- Garofalo E, Bruni A, Pelaia C et al. Recognizing, Quantifying and Managing Patient-Ventilator Asynchrony in Invasive and Noninvasive Ventilation. Expert Rev. Respir. Med. 2018; 12 (7), 557-567
